All content on Eyewiki is protected by copyright law and the Terms of Service. This content may not be reproduced, copied, or put into any artificial intelligence program, including large language and generative AI models, without permission from the Academy.
Can-Vac CCC is a novel technique for capsulorhexis. It is safe, simple and useful in challenging cataract cases, particularly intumescent cataract. It is also effective in routine cataract cases. This article describes the surgical procedure and clinical applications of this novel technique.
Cataract surgery is one of the most common surgeries performed worldwide. Ability to perform a safe capsulorhexis is paramount to success in any cataract surgery.[1][2] Historically, many technqiues of performing capsulorhexis has been described in literature.[3][4][5][6][7][8][9][10][11][12][13][14][15][16][17]However, modern day cataract surgeons employ continuous curvilinear capsulorhexis (CCC) as their preferred method.[5][6]
Can-Vac CCC is the latest innovation in the domain of capsulorhexis that is safe, simple and useful to perform in some of the most challenging cataract cases.[18][19]
Principle and Novelty of technique
Principle
Novel Can-Vac CCC uses vacuum suction generated at the cannula tip by the piston of the syringe as the primary mechanism for creating rhexis during cataract surgery.[18][19]
Novelty
A 25-gauge cannula provides an appropriate bore size, just adequate for grasping the free rhexis flap.
The tip which is neither too small nor too large, provides ample suction and does not lead to excessive viscoelastic aspiration or flap amputation respectively.[18][19]
Surgical procedure
Figure 1: Rhexis initiated by raising a flap using 26 gauge cystitome
Instrumentation
A 25 gauge rounded/flat blunt tipped cannula attached to a 5ml syringe is required for Can-Vac CCC.
Surgical steps
Initially a 26 gauge needle cystitome is used to create a nick in the anterior lens capsule and raise a small flap.
The Can-Vac cannula tip is then introduced into the anterior chamber (preferably from the side port incision).
The free edge of the rhexis flap is held with this cannula tip by the suction force generated by manually withdrawing the syringe piston.
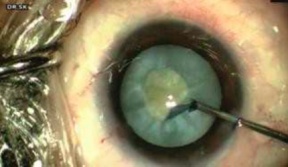
The flap is then grasped and re-grasped by regulating the suction pressure through manual manipulation of the syringe piston. This maneuvre is continued in a circular fashion to create a well formed CCC of desired size.Figure 2: Can-Vac cannula used to grasp the raised flap and make CCC.
Any loose cortex or milky lens fluid (in patients with intumescent cataract) released during the process can be withdrawn by the cannula into the syringe obviating the need for repeated instrumentation and thus helping a clear visual field for surgery.
Figure 3: Can-Vac technique used to continue and complete the CCC.The whole process can be completed in a single step of instrumentation without any need for repeated viscoelastic injection and also avoiding any chamber collapse.
Indications
Intumescent cataract, where there is high intralenticular pressure and risk of Argentina Flag sign and run off rhexis.
Total and hypermature cataract.
Immature cataract.
Advantages
A novel inexpensive technique
Easy availablility
Reusable
Reproducible
Obviates the need for repeated instrumentation including repeated injection of viscoelastics
Lesser chances of chamber fluctuation and risk of rhexis run off
Provides a clear operating field by helping aspiration of the liquefied cortex (in patients with intumescent cataract).
Limitations
Initial technical difficulty with the learning curve.
Additional resources
We suggest the readers to watch the link below to get a visual understanding of this technique.
References
↑Carifi G, Miller MH,
Pitsas C, Zygoura V, Deshmukh RR, Kopsachilis N. Complications and outcomes of
phacoemulsification cataract surgery complicated by anterior capsule tear. Am J
Ophthalmol 2015;159:463‑9.
↑Oner FH, Durak I, Soylev M, Ergin M. Long‑term results of various anterior capsulotomies and radial tears on intraocular lens centration. Ophthalmic Surg Lasers 2001;32:118‑23.
↑Kwitko
M, Simcoe W. Manual extracapsular surgery. In: Marvin L Kwitko, Charles D
Kelman, editor. The history of modern cataract surgery. The Netherlands: Hague;
Kugler publishers; 1998. p. 91-106.
↑Haigh PM, Habib N, King
AJW, David DB. Modified capsulorhexis vs. envelope capsulotomy in extracapsular
cataract surgery. Eur J Implant Refract Surg 1995;7:291‑4.
↑ 5.05.1Gimbel HV, Neuhann T.
Development, advantages, and methods of the continuous circular capsulorhexis
technique. J Cataract Refract Surg 1990;16:31‑7.
↑ Arshinoff S. Mechanics of capsulorhexis. J Cataract Refract Surg 1992;18:623‑8.
↑ Gimbel HV. Two staged capsulorhexis for endocapsular phacoemulsification. J Cataract Refract Surg 1990;16:246‑9.
↑ Pham DT, Liekfeld A, Hartmann C. Capsulotomy in intumescent cataract with the high frequency diathermy capsulotomy. Klin Monbl Augenheilkd 1998;212:29‑31.
↑ Powers MA, Kahook MY. New device for creating a continuous curvilinear capsulorhexis. J Cataract Refract Surg 2014;40:822‑30.
↑ Kranitz K, Takacs A, Mihaltz K. Femtosecond laser capsulotomy and manual continuous curvilinear capsulorrhexis parameters and their effects on intraocular lens centration. J Refract Surg 2011;27:558‑63.
↑ Chang DF, Mammalis N. Precision pulse capsulotomy preclinical safety and performance of a new capsulotomy technology. Ophthalmology 2016;123:255‑64.
↑ Chang DF. Zepto precision pulse capsulotomy: A new automated and disposable capsulotomy technology. Indian J Ophthalmol;65:1411‑4.
↑ 18.018.118.2Kodavoor SK, Deb B, Ramamurthy
D. A Novel Inexpensive Rhexis Technique-Can Vac Ccc for Immature and White
Intumescent Cataract - Our Experience. International Journal of Ophthalmology
& Visual Science 2020;5:53-6.
↑ 19.019.119.2Kodavoor SK, Deb B, Ramamurthy
D. A Novel Inexpensive Rhexis Technique-Can Vac Ccc for Immature and White
Intumescent Cataract - Our Experience. International Journal of Ophthalmology
& Visual Science 2020;5:53-6.
The Academy uses cookies to analyze performance and provide relevant personalized content to users of our website.