All content on Eyewiki is protected by copyright law and the Terms of Service. This content may not be reproduced, copied, or put into any artificial intelligence program, including large language and generative AI models, without permission from the Academy.
Exudative (or serous) retinal detachment (ERD) occurs when fluid accumulates in the subretinal space between the sensory retina and the retinal pigmented epithelium (RPE) resulting in retinal detachment. Causes for fluid accumulation include inflammatory, infectious, and neoplastic diseases of the choroid or retina.[1][2]
Causes
Inflammatory
Serous Retinal Detachment in Vogt-Koyanagi-Harada Disease ODSerous Retinal Detachment in Vogt-Koyanagi-Harada Disease OS Vogt-Koyanagi-Harada (VKH) syndrome
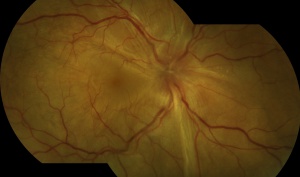
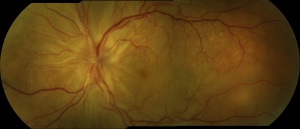
Acute Toxoplasmosis Neuroretinitis By Hamid Ahmadieh, MD. Color fundus photograph of the left eye of a 26-year-old man with clinical picture of acute neuroretinitis and serologic evidence of Toxoplasma gondii infection. Disc swelling, necrotizing retinitis with overlying vitreous inflammation, retinal vasculitis, and localized exudative retinal detachment are visible.Toxoplasmosis
Choroidal MelanomaChoroidal Melanoma By Karen Panzegrau. Ultra-wide field Optos image of a 27-year-old male patient who presented with loss of vision for about 6-8 weeks. Previous choroidal nevus seen. Recommended annual monitoring. No exam for since 10/2014. Brachytherapy vs enucleation was discussed. Brachytherapy was decided as treatment. Full metastatic work up is being performed. Choroidal Melanoma By John T. Thompson, MD. Fundus camera. Amelanotic choroidal melanoma with serous retinal detachment
The subretinal space, a remnant of the embryonic optic vesicle, is practically nonexistent in a healthy eye. However, pathologies that disrupt the integrity of the blood-retina barrier (BRB) can cause leakage of fluid that enlarges the subretinal space and separates the sensory retina from the RPE resulting in retinal detachment.[1]
The BRB has an inner and outer component. The inner blood-retina barrier (iBRB) is composed of tight junctions in between cells of the retinal endothelium whereas the outer blood-retina barrier (oBRB) is composed of tight junctions between cells of the RPE. [3]
Diagnosis
Diagnosis of ERD begins with a detailed history and ophthalmic exam.
History
ERD may develop from localized ocular disease or as a manifestation of wide-spread systemic disease and thus a thorough ocular and medial history is required.[1] Some patients report a progressive, fluctuating loss of peripheral vision. [4]
Physical Exam
Slit-lamp examination, dilated fundoscopy, and indirect ophthalmoscopy with scleral depression should all be performed. ERD can appear as shifting fluid beneath the retina. The fluid shifts with gravity and can change location according to patient position.[4] Exudative detachment looks smooth compared to a jagged, rhegmatogenous detachment.
Diagnostic vitrectomy is crucial for infectious and neoplastic causes of ERD.
Management
Treatment
Unlike rhegmatogenous and tractional detachment which are treated surgically, ERD is generally treated medically. Treatment focuses on the underlying pathology causing the fluid buildup.
Medical
Immunosuppressive
For ERD caused by non-infectious uveitis (e.g. VKH syndrome), common treatment is high dose IV steroids followed by oral steroid taper. Intravitreal triamcinolone has also been used. Alternatives to steroids include cyclosporine A, azathioprine, methotrexate, mycophenolate mofetil and infliximab.[1]
Intravitreal bevacizumab (IVB) can be helpful for subretinal fluid exudation due to its anti-angiogenic and anti-permeability properties.[1]
Other
Eplerenone (mineralocorticoid receptor antagonist) for CSC.[1]
Interventional
Focal laser photocoagulation, cryotherapy, low-dose plaque radiotherapy, photodynamic therapy (PDT) and pars plana vitrectomy (PPV).
Prognosis
Prognosis for ERD is highly variable and heavily dependent on etiology. Acute, self-limited causes of ERD have a favorable prognosis whereas chronic, irreversible causes have a poor prognosis.[1] Prognosis is particularly poor if there is macular involvement and in cases of metastatic and paraneoplastic disease.